Hearing tests
The standard ‘pure tone audiogram’ measures the quietest sound you can hear. You listen through headphones to sounds from a carefully calibrated instrument (audiometer), and respond (e.g. by pressing a button) whenever you hear a sound, however quiet. This is called the threshold of hearing, and measures whether you have a hearing loss. An equally important, but less frequently used test measures the upper limit of loudness tolerance (loudness discomfort levels). You should indicate when the tones become uncomfortable to the ear (before they become painful). For patients who are frightened of loud sounds this test must be done very carefully and with proper instruction by a TRT trained professional. None of the sounds from the audiometer are capable of damaging the ear, even in a sensitive individual. It is very important to have a good knowledge of the level of loud sound tolerance when diagnosing and treating decreased sound tolerance, or when fitting a sound generator or hearing aid to any patient, whether they have hyperacusis or not.
The Limbic System, Emotional Responses and Global Hypersensitivity
Changes in emotional state, particularly mood fluctuations or anxiety can increase overall arousal and make us more able to detect potential threats in our environment. This is a normal protective mechanism. These emotional changes can also increase the apparent loudness and irritation of sounds to which we are already hypersensitive. In some people this results in a “global” hypersensitivity where all stimuli, be it vision, touch, heat, smell, taste or pain are increased greatly in their perceived intensity.
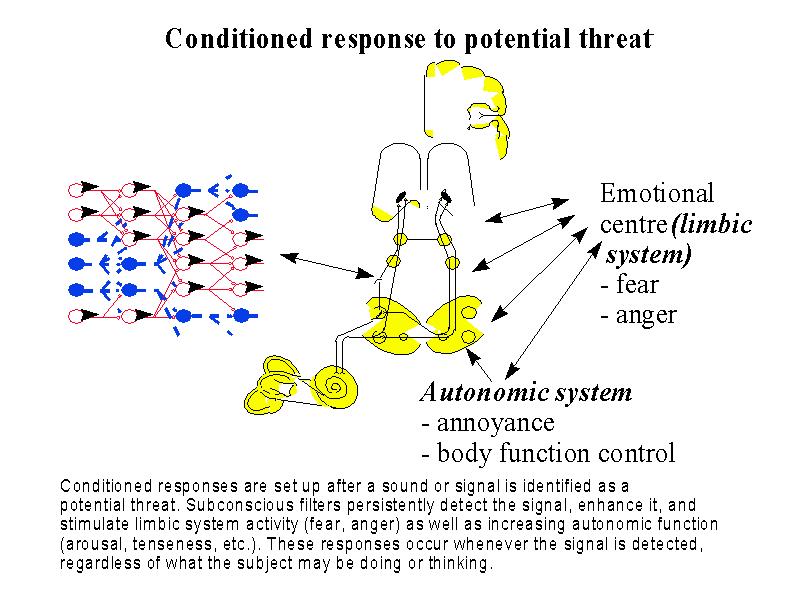
The process of developing an increased sensitivity to specific sound always involves the limbic system and autonomic nervous system. Where phonophobia or misophonia exists there is an inevitable association of fear or dislike, associated with the appearance of the sound, whenever it occurs. The attentional focus becomes filled with that sound, so that interference with concentration (on another task) occurs. These conditioned responses act like survival reflexes and have to carry a message of unpleasant emotion, in order to ensure that a response occurs. They also stimulate the autonomic nervous system to prepare us for ‘flight or fight’ so there may be coincident increases in heart rate, sweating, muscle tension, and other adrenaline-mediated body responses. Check Figure 2 again.
Treatment of Hyperacusis with hearing loss
Where there is a hearing loss and a need for a hearing aid fitting, this must be done without overloading the ear with amplified sound. Nearly all hearing aids have some form of compression,which stops loud sounds entering the hearing aid from being over-amplified.
Digital and programmable hearing aids frequently make the task of appropriate hearing aid fitting easier and more appropriate. In fitting hearing aids to sensitive ears, it is often best to leave the ear canal as un-occluded as possible, particularly to begin with.
Avoidance of silence
Many people seek silence as a way to escape from the pressures of everyday life. However complete silence is not found in nature, and should be considered ‘unnatural’. Consider living in a nest or animal burrow! In the relative silence of houses with doubled-glazed windows, often hermetically sealed from the outside world, the absence of sound stimulation leads to an increase in auditory gain (amplification) in the subconscious auditory pathways. The brain is always looking the best way it can for auditory signals. This process is enhanced by silence which is considered to be one of the signs of possible predator activity . The auditory filters ‘open’ in an attempt to monitor the external sound environment. External sounds may then increase dramatically in their perceived intensity and intrusiveness. Some people take to wearing ear plugs, perhaps at night, to avoid sounds becoming intrusive, and this simply worsens the sensitivity. When hyperacusis develops there is a great temptation to plug the ear to exclude unwelcome sounds. This is actually making things worse, as it encourages further increase in the amplification of sounds on their way to the auditory (hearing) cortex. When these sounds are heard in the absence of plugs, their perceived loudness is greatly increased.
The part of the treatment is always a directive counselling, or retraining approach designed to remove the need to plug or otherwise protect the ear from normal levels of environmental sound..It is understandably difficult to accept that sound which can be uncomfortable or even painful to the HEARING, can be quite harmless to the EAR. A complete understanding of the Jastreboff model is necessary for both professional and subsequently the patient. The retraining must be undertaken by professionals trained in TRT. Hearing conservation remains important in proven damaging noise situations, (e.g. gunshot, discos, industrial machinery etc) and here appropriate protection with muffs or plugs is needed, but only when in these environments.
Damage is related not only to the intensity of sound, but also to the duration of exposure, so careful calculations need to be made to establish who is really at risk.
Wearable Sound Generators (WSGs / WNGs)
Research in the 1980s (Hazell & Sheldrake1991) showed that the use of wide band noise applied to the ear by wearable sound generators can in help in the treatment of abnormal hypersensitivity of hearing. This is particularly true in hyperacusis, where on some occasions, particularly in young children, it is all the treatment required.
The sound from the instruments needs to be applied very gently and gradually to the ear beginning at a low level, always to both ears, and under the supervision of an audiologist with experience in this process of desensitization and with training in TRT. The effect, which in some cases may be quite dramatic, results in a ‘turning down’ of central auditory gain and a reduced perception of loudness for previously distressing sounds. Over a period of months, due to changes in the auditory neuronal networks, there is a permanent change in loudness discomfort, which can be demonstrated by audiometric testing of loudness discomfort levels. In patients where a severe increase of symptoms occurs, which genuinely persists after a good nights sleep, very careful use of sound therapy needs to be applied, under the guidance of an experienced professional. In severe cases there must be a gradual transition from wearing ear plugs to using WSGs. Fortunately WSGs ‘turn down’ the amplification of external sounds, so many people can immediately tolerate sounds which previously were distressing. Never undertake any sound therapy without proper advice. Sound tapes – e.g. pink noise, can make certain hyperacusis and phonophobic patients considerably worse. In each case carefully explanation of the mechanism of central processing must be given, so that individuals can understand and believe what has happened to them, and that the whole process is reversible with time, and the appropriate therapy. Where misophonia (dislike) or phonophobia (fear of sound) exists, no permanent change in discomfort can be achieved without a successful behavioural programme aimed at reversing inappropriate beliefs responsible for the conditioned aversive response. This is true for any phobia (e.g. claustrophobia, arachnophobia, fear of heights etc). The whole process of desensitization can take quite a long time, commonly six months to a year, but is achievable in most cases. In rare cases where phonophobia is present alone without any hyperacusis, WSGs are not indicated.